Pollen 101: how nurses can help patients manage hay fever symptoms

Hay fever rates have grown more than three-fold since the 1970s, and the condition now affects more than a quarter of UK adults. Health journalist Rebecca Seal explores the science behind pollen allergies, their wider health impacts, and what nurses can do to help patients manage their symptoms more effectively.
Pollen allergy was first identified in 1859 by a Manchester-based doctor called Charles Blackley.1 A sufferer of the ‘summer catarrh’ himself, he wanted to know what was causing his symptoms and spent years inhaling different substances, scratch testing his own skin and dropping irritants into his eyes to find the culprit.
It was only when a passing horse and cart covered him in dust one summer’s day, causing an hours-long sneezing fit, that he put the dust under a microscope and finally identified his trigger as grass pollen.
Unfortunately, Blackley’s findings weren’t widely accepted until after his death at the end of the century. This was partly because hay fever was so rare at the time that Blackley had no choice but to conduct most of his experiments on himself.
Therefore, until the early 1900s, people continued to believe that hay fever was caused by the scent of freshly cut hay – which is where the name hay fever comes from.
Today, however, Blackley would have no trouble finding people with pollen allergies for his experiments as around 26% of adults and 10-15% of children in the UK have a pollen allergy.2
How pollen triggers the allergic cascade
Hay fever – or seasonal allergic rhinitis – is an IgE-mediated allergy and symptoms are primarily experienced in the nasal passages, eyes and respiratory system. Reactions occur when pollen is released into the air by plants and makes contact with the epithelial layer of the eyes, nose or lungs of a person with an allergy to that specific pollen.
When this happens, the immune system is activated, causing mast cells to release histamine and other inflammatory or signalling chemicals, which then trigger local swelling, redness, irritation, sneezing, excess mucus production and sometimes coughing.
Hay fever usually doesn’t cause life-threatening anaphylaxis, but there have been cases of people with hay fever experiencing anaphylaxis after eating bee pollen, royal jelly and – much more rarely – honey.3
Exactly when an individual’s hay fever symptoms will start each year depends on which tree, grass, weed or flower pollens they are sensitised to. Pollen season can start as early as January when alder, hazels and yews start producing pollen and it can continue well into October, when ragweed is still active.4
Why does hay fever seem to be getting worse?
It’s not a myth that hay fever starts earlier and affects more people more severely than it did in the past. Climate change has been shown to elongate the pollen season,5 while elevated carbon dioxide levels appear to intensify it by driving plants to produce more pollen.
In addition, some types of air pollution or stress – such as sulphur dioxide, nitrogen dioxide, ammonia, vehicle exhaust particles or drought – induce plants to generate pollen grains that are more densely packed with allergenic proteins.6,7
Moreover, some polluting chemicals, such as ozone, may break airborne pollen into smaller fragments that can then travel much deeper into the lungs, causing even more symptoms.8
Male trees produce more pollen than females, but until very recently they were preferred in urban landscaping as they create less litter.9 This has resulted in many parks and school playgrounds being dominated by male birch trees and grasses, which generate huge amounts of airborne pollen.
Co-morbidities and complications
Anything that intensifies respiratory inflammation can worsen hay fever symptoms, particularly if the underlying conditions aren’t properly diagnosed and managed.
People with hay fever are four times more likely to have asthma, eczema, food allergies, and other forms of allergic rhinitis – such as reactions to dust mites, pet dander, or indoor and outdoor moulds.10
Living in a polluted urban environment or in a home with lots of indoor pollution from things like cooking, vaping, and candles can also irritate the lungs, eyes and nasal passages and exacerbate rhinitis symptoms.11,12
Asthma
Around four out of five people with asthma also have allergies.13 Pollen-triggered allergic asthma that is not well controlled can be very dangerous when the pollen count is high, with data showing that London hospital admissions for asthma may go up by around 46% in the days immediately after the grass pollen count is elevated.13
Eczema
If someone has hay fever and eczema, pollen can irritate the skin and cause itching. Some studies have even suggested that if pollen enters the body through broken skin, eczema might help hay fever develop – especially in allergy-prone babies and young children.14,15
Therefore, it is extremely important that people get good advice on eczema management if they have co-morbid hay fever.
Pollen food syndrome
While pollen food syndrome (PFS) affects around 2% of the general population, some studies have shown it impacts around 66% of adults with a birch pollen allergy.16
Also known as oral allergy syndrome, PFS happens when the body mistakes a raw plant protein in a food for a pollen protein to which it is allergic and cross-reacts to it when the protein is eaten.
PFS usually causes relatively mild symptoms like itching and swelling in the mouth and throat, or contact reactions on the hands, and it rarely causes anaphylaxis.
Although it usually resolves on its own or with antihistamines, some people need to carry adrenaline auto-injector to deal with more serious PFS reactions.
Impact on sleep, cognition and mental health
Hay fever is often called a mild allergy, but this is a misnomer. It is a long-term, chronic health condition that can seriously impact wellbeing. Nasal and respiratory symptoms can interrupt or prevent sleep, and feeling puffy, snotty, miserable and blocked up can make socialising very unappealing, especially if it’s outdoors during pollen season.
Poor sleep and hay fever symptoms can affect a person’s ability to work or learn, and a large study of over 92,000 students in Finland showed that results are lower if exams are taken during pollen season.10
There is even evidence that hay fever and high pollen counts might be connected to suicidal ideation and suicide attempts, perhaps because of the way pollen allergy interacts with certain chemicals in the brain,17 sleep deprivation, or because of hay fever symptoms themselves.13
The role of nurses
There are a wide range of things that community and practice nurses can do to help people with pollen allergies. Crucially, it is important that people understand that hay fever is a health condition and that those with it don’t have to put up with symptoms or rely solely on over-the-counter treatments.
Clinical advice
Treatments
- First-generation sedating antihistamines such as chlorphenamine are generally not recommended for respiratory allergies
- Patients with hay fever often need to try a range of second-generation non-sedating antihistamines, such as loratadine, fexofenadine and cetirizine, before finding the one that works best for them.
- Although second generation anti-histamines are typically classed as non-sedating, they can still cause drowsiness in some individuals.
- Patients should start hay fever medications a few weeks before the beginning of their particular pollen season, as this can stop or reduce symptoms.
- Antihistamine eye drops containing active ingredients like sodium cromoglycate, can do a lot to calm local irritation and may work faster than oral medicines.
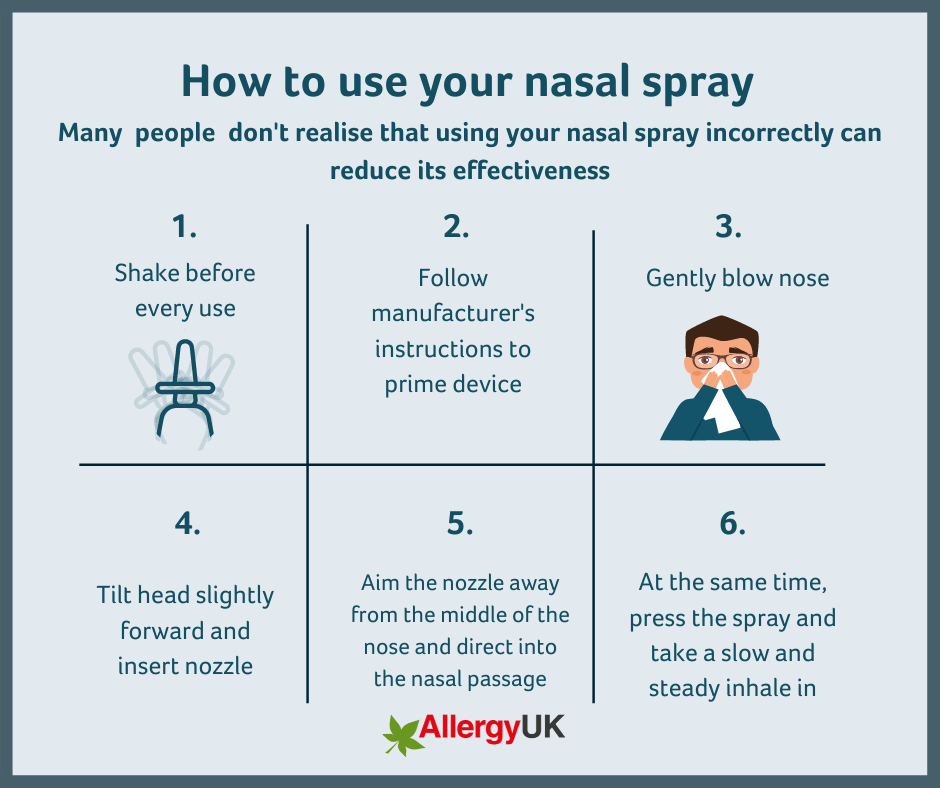
- For moderate-to-severe symptoms, intranasal corticosteroid sprays are generally the most effective treatment. Some patients may benefit from combining these with an antihistamine nasal spray if symptoms remain uncontrolled.
- Some benefit from corticosteroid nasal sprays may be noticed within several hours, but these products often take a few days of regular use to achieve their full effect. Like oral treatments, they need to be used consistently throughout the pollen season.
- Many people buy or are prescribed nasal sprays without being taught how to use them properly. In these cases, patients either aim the spray incorrectly, or sniff immediately after using it, which draws the medication out of the nasal passages towards the throat, so they swallow the dose before it can have an effect within the nose.
- Patients are often unaware that stronger doses of certain treatments for severe symptoms may be available on prescription.
- Most people with hay fever do not know how to access pollen immunotherapy treatments for severe symptoms.
Non-pharmacological recommendations
- When pollen counts are high, people should:
- Change clothing and shower on arrival home
- Avoid leaving clothes or bedding outside to dry
- Keep windows closed
- Wear wrap-around sunglasses outside
- Try to prevent pets bringing pollen into the home on feet and fur
- Applying a small amount of petroleum jelly or lip balm around the nostrils may help trap some pollen before it is inhaled.
- Air purifiers and vacuum cleaners fitted with HEPA filters can help with hay fever symptoms and sleep – especially if they have hay fever alongside asthma or other environmental allergies.
Rebecca Seal is the author of Irritated: The Allergy Epidemic and What We Can Do About It, published by Headline Home, £22.
Resources
- Allergy UK. How to use a nasal spray. https://www.allergyuk.org/wp-content/uploads/2022/06/Nasal-Spray.png
- Pollen calendar. https://www.kleenex.co.uk/advice/pollen/pollen-calendar
- Met Office. Pollen forecast. https://weather.metoffice.gov.uk/warnings-and-advice/seasonal-advice/pollen-forecast#?date=2026-06-03
References
- Darwin Correspondence Project. Charles Harrison Blackley. https://darwinproject.ac.uk/charles-harrison-blackley
- Allergy UK. Statistics and figures. https://www.allergyuk.org/about-us/media-centre/statistics-and-figures/
- Jarlot-Chevaux S, et al. Anaphylaxis to bee products: About 32 cases reported to the French Allergy-Vigilance Network. Rev Fr Allergol 2022; 62: 158-165.
- Pollen calendar. https://www.kleenex.co.uk/advice/pollen/pollen-calendar
- Anderegg W RL, et. Anthropogenic climate change is worsening North American pollen seasons. Proc Natl Acad Sci USA 2021; 118:
- Juprasong Y, Songnuan W. Plant Stress Scenarios Differentially Affect Expression and IgE Reactivity of Grass Group-1 Allergen (β-Expansin) in Maize and Rice Pollen. Front Allergy 2022; 3: 807387.
- UK. Air pollution and airborne allergens. https://www.gov.uk/guidance/air-pollution-and-airborne-allergens
- Sedghy F, et al. Interaction Between Air Pollutants and Pollen Grains: The Role on the Rising Trend in Allergy. Rep Biochem Mol Biol 2018; 6: 219-224.
- Allergy UK. Tree planting, air quality, global warming and their exponential impact on allergic rhinitis (AR) and asthma. https://www.allergyuk.org/wp-content/uploads/2021/10/The_Walk_To_School_TH8A91_1_original.pdf
- Davis C M, et al. Health disparities in allergic and immunologic conditions in racial and ethnic underserved populations: A work group report of the AAAAI committee on the underserved. J Allergy Clin Immunol 2021; 147: 1579–93.
- Gledson A, et al. A comparison of experience sampled hay fever symptom severity across rural and urban areas of the UK. Sci Rep 2023; 13: 3060.
- Martinez-Perez C, Oliveira AP. Air Pollution, Pollen, and Indoor Exposures in Allergic Conjunctivitis: A Systematic Review. Life (Basel) 2026;16:
- Osborne NJ, et al. Pollen exposure and hospitalization due to asthma exacerbations: Daily time series in a European city. Int J Biometeorol 2017; 61: 1837–48.
- Biagini Myers JM, Khurana Hershey GK. Eczema in early life: genetics, the skin barrier, and lessons learned from birth cohort studies. J Pediatr 2010; 157: 704-14.
- National Eczema Association. The Atopic March: How Eczema Can Lead to Allergies and Asthma. https://nationaleczema.org/blog/science-atopic-march/
- Hugg TT, et al. Pollen exposure and matriculation exam performance among students in Finland. J Epidemiol Community Health 2026; 80: 287-293.
- Abramowitz J, et al. Seasonal allergies and mental health: Do small health shocks affect suicidality? J Health Econ 2025; 104:
See how our symptom tool can help you make better sense of patient presentations
Click here to search a symptom



{kind=link}